
Leprosy
Leprosy, also known as Hansen's disease, is a devastating chronic infectious disease caused by Mycobacterium leprae and Mycobacterium lepromatus. The disease predominantly affects the skin and peripheral nerves. Left untreated, it may cause progressive and permanent disabilities.
The bacteria are transmitted via droplets from the nose and mouth during close, prolonged and frequent contacts with untreated cases. Leprosy is curable with Multiple Drug Therapy (MDT). The patient stops transmitting the disease when they begin treatment.
In 2024, a total of 172 717 new cases of leprosy were reported across all six WHO regions. Of these, 19 171 new cases (11.1%) were reported in the African region, ranking third after the South-East Asia Region (SEAR) and the Americas Region (AMR). The most vulnerable and high-risk populations are living in the Democratic Republic of Congo, Ethiopia, Madagascar, Mozambique, Nigeria and Tanzania, which together reported more than 1 000 new cases each.
People affected by leprosy are often subject to discrimination and stigmatization.

Supporting countries endemic for leprosy
WHO provides technical support to Member States through conduct of situational assessments and programmatic reviews, capacity‐building and advocacy.

Monitoring the leprosy situation
Every year, WHO collates epidemiological data on leprosy from all its Member States and publishes a consolidated report in the Weekly Epidemiological Record. The data including key indicators provided by countries are published in the Global Health Observatory (GHO).
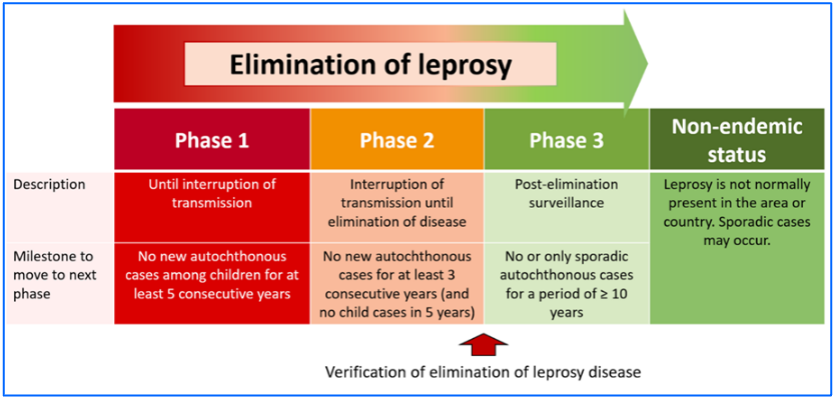
The WHO closely monitors countries' efforts to sustain leprosy elimination as public health problem as well as progress towards interruption of transmission and elimination leprosy disease.
Facilitating the provision of medicines for leprosy
 Multiple Drug Therapy (MDT), a combination of three medicines (dapsone, clofazimine and rifampicin) has been the cornerstone of leprosy treatment since the 1980s.
Multiple Drug Therapy (MDT), a combination of three medicines (dapsone, clofazimine and rifampicin) has been the cornerstone of leprosy treatment since the 1980s.
WHO has facilitated the provision of MDT medicines worldwide and free-of-charge through a donation financed by The Nippon Foundation (from 1995 to 1999) and since year 2000 onwards by Novartis.
Annual Request for the supply of free anti-leprosy medicines
Promoting advocacy and partner coordination for leprosy elimination

For many years, leprosy elimination interventions in countries as well as at the international level have benefitted from dedicated and engaged partners such as the International Federation of Anti-Leprosy Associations (ILEP) and its members; the International Leprosy Association (ILA); The Nippon Foundation (TNF) and Sasakawa Health Foundation (SHF); Novartis; the Leprosy Research Initiative (LRI); and organizations representing persons who have experienced or are affected by leprosy.
WHO has been critical in mobilizing various partners, in countries as well as internationally, to capitalize on their strengths and comparative advantage.
In July 2024, WHO AFRO organized a virtual regional consultation on leprosy elimination in Africa. The discussion focused on the interruption of transmission and elimination of leprosy disease in collaboration with national programs and stakeholders. This effort aims to support countries in enhancing leprosy elimination initiatives and strengthening surveillance activities to meet the 2030 targets.
Since May 2001, WHO has also counted on Mr Yohei Sasakawa, the WHO Goodwill Ambassador for Leprosy Elimination and Chairman of The Nippon Foundation, who has travelled around the world to advocate for the leprosy elimination.
- Sasakawa Health Foundation
- Novartis − Corporate responsibility
- The International Federation of Anti-Leprosy Associations (ILEP)
- International Leprosy Association (ILA)
- Leprosy Research Initiative
- UN Special Rapporteur on the elimination of discrimination against persons affected by leprosy and their family members
Publishing state-of-the art guidance to reduce the leprosy burden
WHO publishes guides and tools to support translation of WHO recommendations into practice. These resources are intended for use by national programmes and partners to support planning, implementing, monitoring and evaluating activities to further reduce the leprosy burden.
In recent years, WHO has published the following guidance documents:
-
- Interruption of transmission and elimination of leprosy disease (2023)
- Towards zero leprosy: global leprosy (Hansen’s disease) strategy 2021–2030 (2021)
- Leprosy/Hansen disease: contact tracing and post-exposure prophylaxis: technical guidance (2020).
- Leprosy Hansen disease: management of reactions and prevention of disabilities: technical guidance (2020).
- Guidelines for the diagnosis, treatment and prevention of leprosy (2018)
- A guide for surveillance of antimicrobial resistance in leprosy: 2017 update
Promoting the integrated approach to skin-related neglected tropical diseases
 Skin diseases are the third most prevalent cause of illness and one of the top 10 causes of disability. They are also among the 10 most common causes of outpatient visits.
Skin diseases are the third most prevalent cause of illness and one of the top 10 causes of disability. They are also among the 10 most common causes of outpatient visits.
Of the 20 neglected tropical diseases (NTDs), more than half present with skin manifestations (the so‐called skin NTDs) and are often associated with long-term disability, stigmatization and mental health problems. The skin NTDs include Buruli ulcer, cutaneous leishmaniasis, post-kala azar dermal leishmaniasis, leprosy, lymphatic filariasis (lymphoedema and hydrocele), mycetoma, onchocerciasis, scabies, yaws, and fungal diseases. They all require similar detection and case-management approaches that present opportunities for integration, which both increases cost–effectiveness and expands coverage.
The major areas in which integrated approaches can be developed include community awareness, epidemiological surveillance and disease mapping, training for health workers and community health workers, active case finding and programme monitoring and evaluation.
In areas of treatment, common approaches such as wound and lymphoedema management, prevention of disability, surgery and rehabilitation can be implemented using the same health infrastructure and health workers. Most nongovernmental organizations and health professional organizations are involved in multiple skin NTDs.
WHO has recently published a Strategic framework for integrated control and management of skin-related neglected tropical diseases
To ensure efficiency, sustainability and scale, WHO recommends that Leprosy intervention should be integrated within skin NTDs approach adapted to the diseases present in a particular country.

In the African Region, several countries, including but not limited to Angola, Benin, Cameroon, Congo, Côte d’Ivoire, the Democratic Republic of the Congo, South Sudan, and Togo are implementing integrated approach.
 WHO has developed online courses and a Skin App for Android and iOS to assist health workers in the field in the diagnosis of skin NTDs including Leprosy
WHO has developed online courses and a Skin App for Android and iOS to assist health workers in the field in the diagnosis of skin NTDs including Leprosy



Publications
See all
2023 Annual Report: Universal Health Coverage, Communicable and Noncommunicable Diseases (UCN) Cluster, WHO Regional Office for Africa
This is the second progress report produced by the Universal Health Coverage, Communicable and Noncommunicable Diseases (UCN) Cluster of the World Health Organization (WHO) Regional Office for Africa.





