
Human African Trypanosomiasis
Sleeping sickness threatens millions of people in 36 countries in sub-Saharan Africa. Many of the affected populations live in remote rural areas with limited access to adequate health services, which complicates the surveillance and therefore the diagnosis and treatment of cases. In addition, displacement of populations, war and poverty are important factors that facilitate transmission.
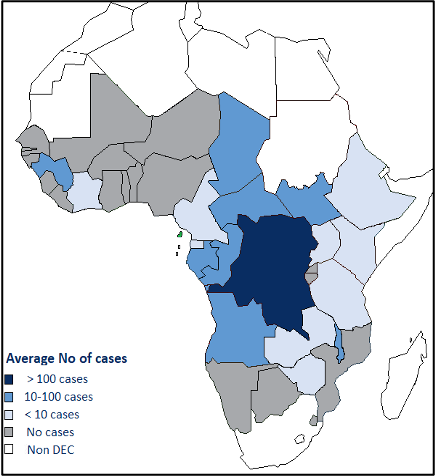
- By the mid-1960s HAT was under control with below 5000 annual cases continent-wide. As surveillance relaxed, a resurgence ensued, reaching epidemic proportions in several regions by 1970. In 1998 almost 40 000 cases were reported, amidst an estimated 300 000 undetected and untreated cases. The prevalence reached 50% in several villages in Angola, the Democratic Republic of the Congo (DRC), and South Sudan. HAT was the first or second greatest cause of mortality in those communities.
- The efforts of WHO, national control programmes, bilateral cooperation, and nongovernmental organizations during the 1990s and early 2000s reversed the curve, and the WHO Neglected Tropical Diseases Roadmap targeted for 2020 its elimination as a public health problem, and for 2030 the interruption of transmission (zero case).
Unspecific symptoms and signs such as headache, fever, weakness, joint pain, and lymphadenopathy appear. Over time, the parasites cross the blood–brain barrier to invade the central nervous system (second stage, meningoencephalitic), causing various neurological disturbances including sleep disorders (excessive daytime sleepiness, nocturnal insomnia), deep sensory disturbances, abnormal movements, tremor, ataxia, walking difficulties, speech difficulties, psychiatric disorders, seizures, coma and ultimately death. Most signs and symptoms are common to both stages, and sleep disorders in particular can appear already during the first stage.
Rhodesiense HAT is typically acute, progressing to second stage within a few weeks, and to death within 6 months. Gambiense HAT progresses slowly over around 3 years (highly variable).
An inoculation chancre (dermal reaction of 3–4 cm at the tsetse bite site) may appear 2–3 days after infection with rhodesiense HAT in up to 25% of local patients, but more frequently in patients from non-endemic regions. It is rare with gambiense HAT.
Sleeping sickness is diagnosed in several steps: after a clinical suspicion, serological tests (card agglutination trypanosomiasis test or HAT rapid diagnostic tests) can reinforce the suspicion, which should be confirmed by parasitological findings (in chancre exudate, lymphatic juice, blood, and cerebrospinal fluid). Unfortunately, the usual serological tests are only applicable to T. b. gambiense. Stage is determined by the number of white blood cells and the presence of trypanosomes in cerebrospinal fluid examination.
All confirmed HAT cases require treatment. Available treatment can cure most patients, completely eliminating trypanosomes from the body. Treatment of cases suspected by serology depends on specific conditions set by national protocols, which usually set specific conditions defining a higher suspicion index.
The current treatment options include six medicines, all of which are donated by the manufacturers; WHO ensures their worldwide distribution free of charge.
Treatment choices are based on the causative trypanosome and the disease stage. The medicines for treatment of second stage must cross the blood–brain barrier and tend to be more toxic and complex to administer than first-stage medicines.
In 2024, WHO issued the guidelines for the treatment of human African trypanosomiasis.
Gambiense HAT can be treated with oral fexinidazole in first-stage and also non-severe second-stage, with some limitations of age and body weight and following some important specific rules to ensure efficacy. In first-stage, intramuscular pentamidine can be also used, and in second stage nifurtimox–eflornithine combination therapy (NECT).
Rhodesiense HAT must be treated without delay, because it can provoke multi-organ failure and progress to second stage within a few weeks. The recommended treatment is fexinidazole in first stage and second-stage. As second line and children below 6 years or less than 200 kg of body weight intravenous suramin is recommended in first stage, and intravenous melarsoprol in second stage.
In the absence of a vaccine or chemoprophylaxis, human African trypanosomiasis is controlled through case detection and treatment, and, to a lesser extent, vector control.
For T brucei gambiense human African trypanosomiasis, the most effective control strategy is case finding and treatment, which reduces the human reservoir and thus decreases parasite transmission.
Cases of T brucei gambiense disease are detected through active screening campaigns by mobile teams, consisting of up to eight people travelling in four-wheel drive vehicles or boats, and through passive screening in fixed health structures.
This labour-intensive strategy is no longer cost-effective in the numerous low-prevalence settings. In low-prevalence settings, targeted door to-door surveys focused on the immediate vicinities of former patients with human African trypanosomiasis may provide an alternative to mass screening and complement passive case detection.
Active screening can also be performed by so-called light mobile teams, consisting of one or two people travelling on motorbikes, who can reach villages or camps that are inaccessible to four-wheel drive vehicles. In the current elimination context, it is also crucial to reinforce passive surveillance, integrating it into the general health-care system and focusing on self-presenting patients.
Because passive surveillance relies on clinical suspicion followed by serological tests, it mostly detects patients with second-stage disease, who are likely to have fed the transmission cycle for years before detection. It is therefore necessary to carry out reactive screening campaigns in the probable areas of infection of these patients.

Publications
See all
Report of the second WHO stakeholders meeting on gambiense human African trypanosomiasis elimination Geneva, 21–23 March 2016
Publication details African trypanosomiasis Number of pages: iv, 54 p. Publication date: December 2016 Languages: English ISBN: 978 9…


